Every so often someone tells me a story that begins like this:
“My heart suddenly started racing. It felt irregular, like it was skipping around. I thought it was anxiety… but something didn’t feel right.”
I’ve heard that exact sentence more times than I can count. Sometimes it is anxiety. But sometimes it’s atrial fibrillation, commonly called AFib. Once I called an ambulance for someone in my pharmacy who was experiencing heart problems, which I recognized as AFib. They came in time and it was a happy ending for the family.
AFib is actually very common. And it’s easy to spot it once you know what to look for that’s why I wrote this article. I want to help you recognize it quickly because that’s critical. AFib is relatively easy to fix and resolve, but if it’s left untreated and you don’t recognize it, or you ignore it, it could lead to a stroke. So please read on.
Its prevalence increases sharply with age, meaning a 25 year old is much less likely to have it occur than a 55 year old.
Studies estimate that more than 4% of people over age 60 have it. But once you understand what’s happening – and why doctors treat it the way they do – it becomes far less mysterious.
Let’s walk through it clearly.
 What Atrial Fibrillation Actually Is
What Atrial Fibrillation Actually Is
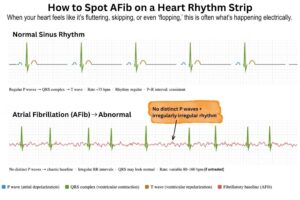
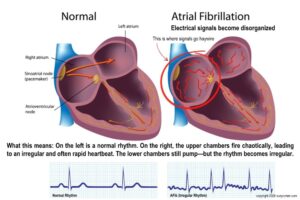
Your heart normally beats in a coordinated rhythm because electrical signals travel through it in an organized pattern.
In atrial fibrillation, the electrical activity in the upper chambers of the heart (the atria) becomes chaotic. Instead of contracting normally, the atria quiver or fibrillate. This causes two things to happen:
- The heartbeat becomes irregular
- The heart rate may also become very fast
Instead of a steady rhythm, the pulse becomes what cardiologists describe as “irregularly irregular.” Some people experience episodes that come and go. It’s called paroxysmal AFib, which simply means the irregular rhythm typically reverts to normal on its own within seven days.
What AFib Feels Like
I’ve not had this so I can’t speak from personal experience, however, these are the most common symptoms reported:
• rapid or pounding heartbeat
• fluttering sensation in the chest
• shortness of breath
• dizziness or lightheadedness
• fatigue or weakness
• reduced exercise tolerance
Many people describe the sensation as though “a fish was flopping in my chest.”
In some cases, the heart rate may rise to 160–180 beats per minute, which is often what brings you to the emergency room. Interestingly, research shows many AFib episodes are silent, meaning they occur without any symptoms! This is why some people discover the condition only during a routine exam or after a smartwatch alerts them to an irregular pulse.
When Should You Seek Medical Care?
If you experience a sudden irregular or fast heartbeat, it’s worth being evaluated. Seek emergency care if you experience any of this:
• a very rapid heart rate
• chest pain
• shortness of breath
• fainting or near-fainting
• severe dizziness
Even if symptoms improve, a first episode of AFib should be evaluated by a healthcare professional. The reason is simple: AFib isn’t just about symptoms. It’s about stroke risk.

AFib Can Lead to Stroke
The biggest concern with AFib is blood clots. When the atria are quivering instead of contracting normally, blood can pool in a small pouch of the heart called the left atrial appendage. When blood sits still, it can form a clot.
If that clot travels to the brain, it can block an artery and cause a stroke.
What Happens in the Emergency Room
When someone arrives in the ER with AFib and a rapid heart rate, the first priority is often rate control. In other words, doctors try to bring the number of beats per minute down to a safer level.
Doctors commonly use medications such as diltiazem or metoprolol, two well-established drugs that slow conduction through the heart’s atrioventricular (AV) node. These medications are often given IV in the emergency room so they can start to work quickly (like within minutes).
But the important point is

that they don’t necessarily stop the AFib itself. You’d think they would but they don’t.
Instead, they slow the pulse from something like 170–180 beats per minute down to a safer range, often around 90–100 beats per minute. This helps stabilize the patient and reduce symptoms such as dizziness, shortness of breath, or chest discomfort.
 Once the heart rate is controlled and you’re stable, you’re doctor will decide whether to:
Once the heart rate is controlled and you’re stable, you’re doctor will decide whether to:
• Allow your heart rhythm to convert naturally, which it often does in cases of paroxysmal AFib (sometimes within a few hours or within the first day). They’ll send you home and you just wait for it to convert back to normal.
• Use medications to restore normal rhythm, such as antiarrhythmic drugs like amiodarone, flecainide, or propafenone, depending on the situation. This is the more likely situation if you go to the E.R. They’ll send you home with the medication, or call it to the pharmacy. Most people will get an anticoagulant as part of treatment. See below for more on those.
• Do electrical cardioversion, a brief procedure that delivers a controlled electrical shock to restore normal rhythm.
Many patients with paroxysmal AFib can go home the same day with follow-up care arranged, especially if their symptoms improve and their stroke risk has been assessed.
So in essence, you go to the ER with the problem, they slow things down. You feel better, you’re safer, then you go home and wait for the rhythm to convert. This is the best case scenario and what happens to most people. I say this because I think some of you may delay seeking medical attention with the assumption that if you go to the E.R. they’re going to crack open your chest, do open heart surgery, or implant a pacemaker… stuff like that. And so no, that’s not going to happen so don’t worry and don’t delay getting yourself help.
A landmark study called the AFFIRM trial found that controlling heart rate can be just as effective as trying to force the heart back into a normal rhythm for many patients.
Why Doctors Prescribe Oral Anticoagulants
Blood thinners reduce the chance that a clot will form and travel to the brain. These are almost always prescribed for a person who has AFib. The most common oral anticoagulants today include:
• ELIQUIS (apixaban)
• Xarelto (rivaroxaban)
• Pradaxa (dabigatran)
• Coumadin (warfarin) –> This older medication is used less often today because it requires frequent monitoring, has a higher bleeding risk, and comes with dietary restrictions (like no salad for example).
A landmark clinical trial called the ARISTOTLE STUDY found that apixaban reduced stroke and major bleeding compared with warfarin in patients with atrial fibrillation.
These medications do not dissolve existing clots. Instead, they reduce the blood’s tendency to form dangerous ones.
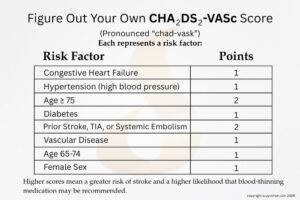
Understanding the CHA₂DS₂-VASc Score
Doctors use a risk assessment tool called the CHA₂DS₂-VASc score to estimate stroke risk. When spoken aloud, it’s usually pronounced “chad-vasc.” Here’s a graphic I made for you so you can calculate your own chad-vasc score. I think it will offer insight into why some people are treated more aggressively with blood-thinners while others are not.
General guideline thresholds (ACC/AHA/ESC)
Take the test now, see what your score is. This scoring system is widely used in cardiology guidelines to determine who should take blood thinners. A lower score often means a lower stroke risk, so not everyone needs long-term medication. Knowing your number helps take the guesswork out of treatment decisions and gives you more confidence in your care.
For men
-
0 points → anticoagulation usually not recommended
-
1 point → anticoagulation may be considered
-
≥2 points → anticoagulation medications are recommended
For women
-
1 point (female sex only) → no anticoagulation is needed
-
≥2 points → anticoagulation usually recommended
In many cases, people with a chad-vasc score of 0 (for men) or 1 due only to female sex for example, are considered low risk for stroke and wouldn’t necessarily need lifelong treatment with blood thinners. But still, some doctors sometimes prescribe a short course of an anticoagulant after a new AFib episode for a few reasons. And you might wonder why if their score is zero or one.
One reason would be that the atria may remain temporarily “stunned” after an AFib episode, which can briefly increase the chance of clot formation while the heart rhythm stabilizes. And here’s where this gets a little nuanced. If the rhythm was restored using cardioversion (either with medication or an electrical shock), cardiology guidelines do recommend anticoagulation meds for several weeks afterward – it’s just as a precaution.
It’s not forever. The drug they give you will almost always be discontinued after a few weeks (but obviously ask your doctor). Doctors may not know exactly how long the AFib episode was going on before it was detected, so that’s another reason. Like, did you sit there with it for six, eight or even 12 hours before going to the emergency room… or did you go within minutes of it starting. If it may have lasted more than a day or two, a short course of anticoagulation is sometimes used to reduce clot risk during that period.
In people with low “chad vasc” scores, anticoagulant meds are not given lifelong.

Cautions About Aspirin
These medications can be costly, so it’s understandable to ask whether aspirin could do the job instead. While aspirin was used in the past, today we know it’s far less effective than anticoagulants for preventing stroke in AFib. The right choice depends on your personal risk, so it’s a conversation to have with your doctor.
Today, most current cardiologists no longer recommend aspirin alone for stroke prevention in atrial fibrillation. They use one of the oral anticoagulants listed above. The most affordable one if you have to pay with cash is the warfarin.
11 Common Triggers and Risk Factors
Many people assume AFib appears “out of nowhere,” but cardiologists often see patterns behind episodes.
AFib often develops when the heart’s structure or electrical system changes. Aside from aging, here are some common triggers and risk factors that can irritate the heart’s electrical system or make it easier for abnormal rhythms to start. Some of the most frequent include:
- Alcohol use
- Coronary artery disease
- Diabetes
- Electrolyte disturbances (low magnesium, potassium, or dehydration)
- High blood pressure (hypertension)
- High stress or excess adrenaline
- Infection or illness
- Obesity
- PACs (premature atrial beats)
- Sleep apnea
- Thyroid disorders (hyperthyroidism or Graves’ disease is most strongly associated with atrial fibrillation)

Can Wearable Devices Detect AFib?
Smartwatches and wearable heart monitors have become increasingly useful. Devices such as the Apple Watch can detect an irregular pulse pattern and alert users. These devices are not perfect, but they can help identify abnormal rhythms earlier and prompt medical evaluation. Still, a formal diagnosis requires electrocardiography (ECG) or clinical monitoring. A study called VITAL-AF showed that simple ECG screening during routine visits can uncover previously undiagnosed AFib.
Why Sleep Apnea and Alcohol Matter More Than Most People Realize
Two factors repeatedly show up in cardiology clinics when patients develop AFib. A lot of times it’s just the result of sleep apnea, and sometimes from alcohol. Let’s talk about apnea first.
Sleep apnea
In obstructive sleep apnea, breathing repeatedly stops during sleep. This leads to drops in oxygen, a surge in cortisol (a stress hormone), and a sudden blood pressure spike. Over time, this nightly stress can enlarge the left atrium and disrupt electrical stability. Studies consistently show that if you treat your sleep apnea it can reduce AFib recurrence, especially after cardioversion or ablation procedures.
If someone you love snores loudly next to you, always wakes up tired, or has pauses in breathing during sleep that you can hear, I think it’s worth getting a sleep study.
You can do these sleep studies from your own home now. You don’t have to go to a sleep clinic and get all hooked up in wires and sleep in an unfamiliar bed! A lot of people don’t realize that, and therefore never get a sleep apnea study. Because sleep apnea plays such an important role in heart rhythm disorders, it’s worth understanding the different types. You can learn more in my companion article: Understanding the Difference Between Central Sleep Apnea and Obstructive Sleep Apnea.

Alcohol (“holiday heart”)
Drinking too much alcohol has a well-known connection to AFib. Even in people with otherwise healthy hearts, episodes can occur after heavy drinking (or binge), or after a holiday celebration or event where a lot of alcohol is served. This phenomenon is sometimes called holiday heart syndrome.
Alcohol can damage the body in so many ways due to oxidative damage. It can irritate heart cells, alter the balance of your electrolytes and increase adrenaline – all of which are bad for AFib. For people who are prone to AFib, reducing or eliminating alcohol lowers the chance of recurrent episodes. Alcohol can also interfere with sleep in ways many people don’t realize.
If you’d like to understand why a nightcap often leads to restless sleep later in the night, read my article: 8 Surprising Reasons that Alcohol Causes Insomnia.
Supporting Heart Rhythm: Nutrients and Lifestyle Strategies
Medical care always comes first, especially with a condition like AFib, but lifestyle and nutritional factors can still play a supportive role.
Supplements aren’t a replacement for proper treatment, but there are a few nutrients that come up often in discussions about heart health. I like to remember them as “MUT”—magnesium, ubiquinol, and taurine. Think of these as supportive, not corrective, and always something to run by your doctor before adding in.
Magnesium
Magnesium plays a key role in electrical signaling in heart cells.
Low magnesium levels can contribute to palpitations, premature beats and rhythm instability.
Ubiquinol (Active Coenzyme Q10)
CoQ10 or it’s more active sibling “ubiquino) helps support mitochondrial energy production in heart muscle. The heart is one of the most energy-demanding organs in the body, and adequate cellular energy may help maintain normal cardiac function. Did you know there are dozens of popular medications that deplete your stores of CoQ10 putting your heart at risk for problems? Here’s the BIG LIST.
 Taurine
Taurine
Taurine is an amino acid involved in electrolyte balance and calcium signaling in heart cells, both of which play a role in maintaining normal rhythm and stable electrical activity. Some research suggests taurine may support heart rhythm in certain individuals, although more large clinical studies are needed.
Electrolytes and hydration
Adequate hydration and balanced electrolytes are often overlooked, but it doesn’t take much to fall out of balance. Sometimes you forget to drink during the day, or you have coffee (which has a mild diuretic effect). This situation can alter levels of sodium, potassium and magnesium which becomes a problem, and increases risk for AFib.
All of these influence electrical activity in the heart. Maintaining good hydration and electrolyte balance can be especially important during illness, heat exposure, or intense exercise. This article may interest you: 3 Devastating Effects of Heat Cramps, Heat Exhaustion and Heat Stroke
Fish Oil Supplements
Fish oil supplements are widely used for heart health, but their relationship with AFib is a bit more complex.
Omega-3 fatty acids like EPA and DHA can lower triglycerides. However, several large clinical trials (including the STRENGTH study) have shown a small but real increase in atrial fibrillation risk at higher doses.
When I say “high-dose,” I’m talking about 3,000–4,000 mg per day of combined EPA and DHA—the levels used in prescription products and clinical trials, not your typical over-the-counter supplement.
This doesn’t mean fish or standard-dose fish oil is harmful. It just means high-doses aren’t that great for the treatment for AFib.
Questions to Ask Your Doctor if You Have AFib
If you’ve been diagnosed with atrial fibrillation—or think you may have it—it’s helpful to go into your appointment with a few key questions. These can help you understand your personal risk and make informed decisions about treatment.
Here are some good questions to start with:
• What type of AFib do I have?
(AFib can be paroxysmal, persistent, or permanent, and knowing is important because treatment may differ.)
• What is my CHA₂DS₂-VASc score?
Your chad-vasc score estimates your stroke risk and helps determine whether or not you should take a blood thinner.
• Do I need an anticoagulant medication to prevent stroke?
If so, ask about the benefits, risks, and which medication may be best for you. The newer ones may be safer in terms of bleeding risk problems, but they’re also more $$$).
• Should we focus on controlling my heart rate or restoring a normal rhythm?
Some people do well with rate control alone, while others benefit from rhythm treatments.
• Could sleep apnea be contributing to my AFib?
Sleep apnea is a common but often overlooked trigger for atrial fibrillation. 
• Should I be tested for thyroid problems or electrolyte imbalances?
Hormone issues and low minerals such as magnesium or potassium can sometimes affect heart rhythm.
• Would a heart monitor or wearable device help track my episodes?
Short-term monitors or wearable technology can help detect intermittent AFib.
• What lifestyle changes might help reduce episodes?
Ask about alcohol, caffeine, sleep habits, hydration, and stress.
• When should I seek emergency care if symptoms return?
Knowing this ahead of time can help you respond quickly if another episode occurs.
- Would a KardiaMobile device help me?
These handheld devices can capture a quick ECG at home. You can learn more HERE. It helps you document irregular rhythms for your doctor to review.
Summary
Atrial fibrillation can feel alarming when it first occurs, but it’s a common and manageable condition. The more you understand what’s happening, the easier it becomes to work with your doctor on a plan that protects your heart and lowers your stroke risk.
Here’s what really matters:
• seek medical care if your heart suddenly feels fast, irregular, or “off”
• understand your stroke risk by knowing your CHA₂DS₂-VASc score
• follow medical advice about anticoagulation if prescribed—don’t skip doses
Most importantly, AFib isn’t just about a racing heart—it’s about preventing stroke and protecting your brain. With proper evaluation and the right treatment plan, many people live full, active lives.
Once you understand what’s happening, it becomes a lot less scary.

Suzy Cohen, RPh, has been a licensed pharmacist for over 30 years, blending conventional medicine with natural approaches to help people feel better and live healthier. She is the founder of Script Essentials, a supplement company known for targeted, custom-formulated products, some with patented innovations.
With a special focus on thyroid health, functional medicine, and drug-induced nutrient depletion (what she calls “drug muggers”), Suzy is the author of several books including Thyroid Healthy, Drug Muggers, and Diabetes Without Drugs. She also writes a nationally syndicated health column and shares practical, easy-to-understand guidance with readers around the world.
