Depression is just a word to those until they experience it. Then it’s hell.
First let me say I am not a fan of medicating normal, regular sadness that we encounter in our life, such as the melancholy associated with losing a job, or when someone unfriends you, or for hormonal cycles. This does not require prescriptions in my opinion! They’re dolled out anyway at times, very indiscriminately and that is not okay with me. Antidepressants alter brain receptors and hormonal levels, they should be reserved for those people in true need, who are holding on by a thread… who are overcoming urges to commit suicide… not because you had a bad day, or a negative experience with someone. If you’re interested in suicide rate by country, there are statistics HERE that you can look at. Currently, for every 23 men that commit suicide, 7 women do (in the United States).
Life has ups and downs and we shouldn’t always depend on pharma to medicate our way through it for the normal ups and downs. When these natural downs happen you shouldn’t be thinking “I need a drink to distract me from these emotions!” Or “I need a pill to numb myself.”
That’s not a healthy, normal way to live. Ups and downs happen. I think I’m referring to the general mindset of our country that feels compelled to medicate every negative feeling, or every feeling for that matter, negative or positive! Take a pill for this feeling, take one for that, before you know it, you’re on a medication merry-go-round.
Studies have repeatedly shown a direct correlation to healthy levels of vitamin D and happy moods, specifically with SAD (Seasonal Affective Disorder).

That said, there are people who are truly depressed and suppressing non-stop urges to harm themselves. Those people need to be cared for lovingly, gently and with all appropriate therapies available. If that includes prescribed medicine, then so be it. It would be indicated and life-saving potentially in my opinion. Today’s article is really for YOU, or for the care-givers that watch over these people.
I have seen and heard so much judgement from people for taking an antidepressant, as if that somehow makes them weaker! But from my standpoint having worked in rehab facilities where people were suicidal, and having known people who have actually committed suicide, I know that depression is a real illness that is on the rise due to inappropriate recognition and the wrong treatment. I have never felt major depression like this, nor have I ever taken a medication, so I cannot fully claim to understand this the way that you do.
What I can say is I’ve worked in the environment for many years, treated thousands of patients in long-term care facilities and retail, and dispensed the medications used for it. Furthermore, like most of you, I’ve seen firsthand depression with relatives who have dealt with it. For that matter, my brother Danny was an alcoholic for years, and I am certain there was some amount of depression that underpinned it. You can read about how much I loved him, and how helpless😢 I felt in my article, My Brother Was a Secret.
If you’re a caregiver, it’s heartbreaking, because you just don’t know what to do. You depend on doctors and psychiatrists to help your loved one, but as time goes by and you see how nothing seems to work, you feel just as hopeless as your loved one! It’s like a dog chasing the tail (but not at all cute.)
Medication treatment should be based upon the neurotransmitters that are imbalanced. Look at the graphic that I purchased for this article. Think of the neurotransmitters that are deficient in your body (and require restoration) as the bullseye of the target. Think of the darts as the medications prescribed to you.
Doctors tend to throw a dart in the dark by prescribing popular drugs without actually measuring metabolites of neurotransmitters (for example HVA or 5-HIAA) which provide a glimpse behind the curtain. Some antidepressants will work for you, and others will not.
A lot of you don’t realize that antidepressants on the market today target one, two, three or more neurotransmitters. The method of treatment for each person needs to be individualized. You can read more about neurotransmitters in this article entitled St. John’s Wort, Serotonin, and Depression.
CAUTION: Be advised NOT to suddenly discontinue any medication treatment (or omit doses) please be forewarned that sometimes this can precipitate a seizure or other adverse symptoms, so when changing your antidepressants, they have to be carefully and slowly weaned under physician supervision. This could take weeks to months depending on how high your dosage is, and how long you’ve been on something.
That is where I see the biggest problem in our world today. If you take an antidepressant and it misses the bullseye, you’re not going to get better 😞and you might get worse, or experience more ideation. Let me preface this next sentence with this: If medication is the method of treatment you’ve chosen to treat your depression, hitting that bullseye with the correct med could make the difference between life and death.
Each person with depression has a unique fingerprint of neurotransmitters and the imbalance is very personal. That’s why some people with depression also have anxiety, while others don’t. Some people have agoraphobia, while others don’t.
Some people have anxiety and panic associated with their depression, but others don’t. Some have depersonalization or derealization disorder associated with their sadness, while others don’t. And so on. Like I said earlier, medication treatment should be based upon the neurotransmitters that are imbalanced. You can see where I’m going with this. So you can’t just expect an SSRI like Zoloft to work for everyone!
SSRI or SNRI? Which is Better?
So let’s get to it, what do you think is better, an SNRI or an SSRI? Or an MOA inhibitor? The answer is unclear. One category of meds will work great for you, and be an epic fail for your friend.
Why is that?
Because Zoloft (sertraline) works by making serotonin linger longer, and that’s great if you have reduced serotonin activity. But what if that’s not your problem? What if you’re depressed because you have low DHEA, a youth hormone that declines after 40. When you run low on DHEA, you look and feel older. Deficiencies are associated with inferior health.
Speaking of DHEA, it’s actually depleted by cholesterol-reducing drugs. Did you know? If not, you can read about DHEA depletion by statins by CLICKING HERE.
What if it’s low testosterone or estrogen. And what if your levels of serotonin are fine, but you have super low levels of norepinephrine or dopamine? In the latter case, Zoloft would not work, and might be harmful, whereas Wellbutrin (bupropion) would be great!

Catecholamines are Antidepressants
Norepinephrine is not the same thing as serotonin. Norepinephrine is a catecholamine, and a breakdown product of dopamine. Think of these two as feel-good hormones that impart energy and passion. In this case, if you are deficient in norepi or dopamine, you would not respond to an SSRI like Lexapro/Celexa/Paxil/Zoloft and others in that category.
For that matter taking an SSRI would cause a relative deficiency of the dopamine and norepi, making you worse. It’s a see-saw, when one side goes up (serotonin), the other side could go down (dopamine), relatively speaking. Contrarily, what IF serotonin is low and dopamine is high?
Then taking a direct precursor such as the over-the-counter amino acid 5-HTP could help you form more serotonin pretty quickly. This little trick has saved lives and reduced suicidal ideation in some cases. But again, ONLY if the serotonin is low.
What I’m trying to say is that each of you respond to the medication that restores activity of the particular neurotransmitter YOU are deficient in. Not everyone with depression is deficient in one specific chemical.
Think of a target -not everyone with depression has the same bullseye.
Weighted Blankets
Some of you could benefit from a med that raises serotonin, dopamine AND norepinephrine. Remeron (mirtazapine) works in this regard. There are also natural ways to raise serotonin, like a weighted blanket which I wrote about in an article entitled 5 Benefits of Using a Weighted Blanket.
Someone else might need lifting of serotonin and norepinephrine but NOT the dopamine. Effexor (venlafaxine) is an SNRI that does exactly that! FYI, most serotonin is produced in the intestinal tract, so starting with GUT health is important to brain health. I’ve heard the saying that your gut is your second brain, but it’s not really… your gut is your OTHER BRAIN!
The complex neurohormonal and physiological effects of prescribed antidepressant meds have become more clearly defined over the past twenty years or so. There was a time when I was a young pharmacist in the 90’s, when the mechanism of action was barely understood at all.
So in my example today, when the anti-depressant bupropion was introduced in 1989, the specific pharmacologic basis of its clinical effects was not completely known.
Research and patient-populated data over the years has proven that this drug has dual norepinephrine and dopamine reuptake inhibition, but is not associated with serotonergic activity. I love that we have this as an option. In other words, bupropion drives up two different neurotransmitters than the SSRI drugs, which seem to be every doctor’s favorite!
But as some of you already know (because you’ve tried it), SSRIs are not right for everyone. Finding the right medication for you is like finding the key to unlock the door. It’s like hitting the bullseye with the dart! If you found it, that’s fantastic, but if you haven’t, I’m writing this article to mention a few more options. And just so you know, there are tests you can take today to measure metabolites of these neurotransmitter compounds (but not the compounds themselves).
We Are All Individuals
No drug is right for everyone, and I’d like to emphasize that!
The way you experience sadness is different than another person, and also, the baseline levels of hormones in your body are very individualized… furhtermore, genetics and family/social support play crucial roles. That’s why you can’t give Prozac to everyone that’s suffering.
Is Your Antidepressant the Right One for YOU?
One clinical pearl that I’d like to leave you with is this:
One reason that your antidepressant hasn’t helped you is because you’re taking the wrong one for you. You may just need something different that is better suited to your make-up.
This is a serious topic. I know that I have readers today that are in bad shape and feeling isolated and sad. I’m trying to help you and tell you that there is hope. What you need to do is trial and error with some of these medications (and other therapies outside the pill) as there isn’t one magic med.
Parkinson’s and Dopamine
You may not realize that the reduction in dopamine activity that is associated with Parkinonism is also the same dopamine that is involved in depresison. Deficiencies in dopamine are assocaited with both Parkinson’s and depression. So someone else reading this today might not have Parkinson’s but might STILL need assistance in raising dopamine and dopamine only!
You can do that naturally with tyrosine and B6, but let’s say you would like a stronger prescribed medication. For this case, a drug like selegiline might be useful in low doses. It is a an agent most commonly used to help control the symptoms of Parkinson’s disease, however, it is an MAO-B inhibitor.
This enzyme MAO-B breaks down dopamine very quickly, so a drug like selegiline will slow that process down and keep dopamine alive a bit longer.
This can help with symptoms of Parkinson’s and also depression. Dopamine is our passion and reward chemical, it is the hormone that was high when you were a love-struck teenager!
It is the same hormone that is active when you get excited about sex, or when playing slot machines or for some of the ladies, walking into DSW 👠 ha ha! Couldn’t resist... yeah and for others, perhaps watching Monday Night Football 🤣 it’s all dope as in dopamine! Without it life is pretty dull, grey and flat-lined.
Dopamine is a passion hormone that is low in many people with depression, and again, SSRIs do not lift that. Can anyone take selegiline? Of course not, it is specifically useful for people who are low in dopamine and you need to ask your doctor if it’s right for you.
In closing, I couldn’t possibly know what’s right for everyone because neurotransmitter levels are like fingerprints in people. Sometimes depression is caused by folate or B12 deficiency, or thyroid illness. See below. Sometimes it’s from very high inflammatory compounds, or from a biotoxin-like mold. This may surprise you but sometimes it’s medication-induced, like from The Pill.
As it pertains to inflammation, the drug Celebrex (celecoxib) might be helpful in reducing the amount of time that it takes your antidepressant to start working. Loyola University conducted the research. You can read about that HERE.
You Are Loved
My point is primarily to give you hope.
If you feel like you’re at your wits end and you’ve tried everything and it’s just time to go (and stop being a burden to others) then you need to STOP thinking that immediately because it simply isn’t so. You haven’t tried everything. There are people who love you and need you. ❤️
There is so many other things you can try.
National Suicide Prevention Line: 800-273-8255
You can now text as well, text HELLO to 741741
You can connect with a responder if you’re a veteran by CLICKING HERE
Let’s talk about thyroid hormone a minute…
Did you know that there was a huge clinical trial where the researchers proved that giving some thyroid medicine to people who were sad and depressed worked better than the antidepressant drug? True story, this is an easy, cheap medication to get and if you’re depressed and feeling ‘slow and cold’ on top of feeling sad, then this is probably related to low thyroid levels.
You can click HERE to learn more about how stress impacts Hashimoto’s, Graves’ disease and hypothyroidism. Thyroid illness is often misdiagnosed. Please take a moment to read my other article entitled, Hypothyroidism Often Mistaken for OCD, Depression and Anxiety.
Your tests for thyroid hormone might be normal, but just try the thyroid medicine anyway if your doctor agrees that a few weeks is a good trial run for you. Perhaps something like Cytomel (Liothyronine) 25 mcg or a desiccated thyroid like Armour or Nature Throid 1/2 grain once or twice daily. If you take Synthroid and want to convert to desiccated, here’s a handy CONVERSION GUIDE.
Obviously, these are just my ideas, the dosage that is right for you needs to be based upon your T3/T4 and TSH levels, as well as what your physician suggests. My point is thyroid helps and sometimes more than an antidepressant drug! Talk to your doctor about what’s specifically right for your case.
In fact, if thyroid interests you, I have many resources, including this incredible magazine that (when it was available in Costco and Whole Foods) was their #1 selling magazine. I have a few copies here at my website CLICK HERE.
Social support.
Social support is very important and anyone who is depressed (whether they admit it or not) needs your presence, either by text, or phone or visits. Finally, some people don’t like the word “depressed” or admitting that they have “depression.” But there are other signals and phrases they use which could alert you to their loneliness and despair.
So here are ways to tell when someone you care about is hiding under a veil of embarrassment. The following phrases are code for “I’m depressed.” Be on the lookout if you hear any of the following:
* I don’t want to burden you (feeling guilt about requiring care, or not being able to participate)
* I can’t do anything right (feeling guilt about being so absent in another person’s life)Everyone would be better off without me (feeling desperate)
* I can’t go with you, I don’t feel well (better than saying I’m sad and crying right now)
* I want to go home already (they might be talking about their spiritual home)
* I feel like I’m dreaming, like this isn’t real (a clue to depersonalization disorder)
* I’m just afraid of stuff, but I’m not sure why (a clue to high anxiety)
* I’m sorry (sometimes a farewell)
* I don’t care (saying that a lot may indicate apathy)I love you (sometimes a final goodbye)
* I need to talk, can you come over right now (sometimes a call for help, don’t ignore this)
Below are 8 things NOT to say to someone who is depressed
The following statements might come off as possibly annoying, dismissive or not true for the person so don’t say:
- Just think happy thoughts. Count your blessings.
- Your life is so good, look at everything you have there’s nothing to be sad about, let me tell you about my story…
- Everything will be alright, stop worrying so much.
- Stop eating so much sugar (or gluten) it’s bad for you.
- Snap out of it for crying out loud.
- I know so-and-so and he is so much worse than you.
- Let’s not talk about how bad you feel, it isn’t good for your morale.
- You should exercise more, if you did that you’d feel better.
In closing, I’d like to remind you that there are upwards of 30 different types of medications to try, so you haven’t “tried it all” and if you’re willing to test yourself for these neurotransmitters and see what you are specifically low in, your physician would be able to personalize your medication instead of throwing a dart in the dark.
Testing
There are several tests you can take today. One is called OATS and it’s available through your doctor. It stands for “Organic Acids Test” and it’s available by Great Plains. Your physician has to order that one for you. Organic acids are excreted by humans, and in urine they are about 100 times their concentration compared to the blood serum so seeing metabolites of neurotransmitters gives you an indication of levels. You can’t measure the actual neurotransmitters so measuring the Organic Acids is useful instead.
Another TEST is available -one that measures neurotransmitter metabolites such as Organic Acids, as well as your sex hormones (ie testosterone, estradiol, cortisol and many others) is called DUTCH Complete.
See the graphic below. Dopamine becomes Homovanillic Acid (HVA), norepinephrine breaks down into normetanephrine and VMA, and epinephrine becomes metanephrine and VMA. Seeing the amounts of these that spill into your urine are important because if for example, you have extremely low levels of norepinephrine, the medication you choose should be able to inhibit reuptake, or to create more of it.
You can see why analyzing the metabolites which are eliminated from the body in the urine are so critical. It helps you and your doctor put the dart in the bullseye.
You can buy the DUTCH Complete hormone directly through me by CLICKING HERE. You don’t have to. You can certainly ask your physician. I’m just trying to be helpful and remove a kink from the process if you’re in a hurry, or don’t have the time to wait to get in to see him/her.

I’m a licensed pharmacist – a practitioner registered with the lab company- so therefore I’m allowed to offer labs to you directly. (I cannot interpret or read them though because I’m not a doctor) but you can take the results to your own physician and get professional evaluations. There is also an explanation that is included in your test results which are emailed directly to you.
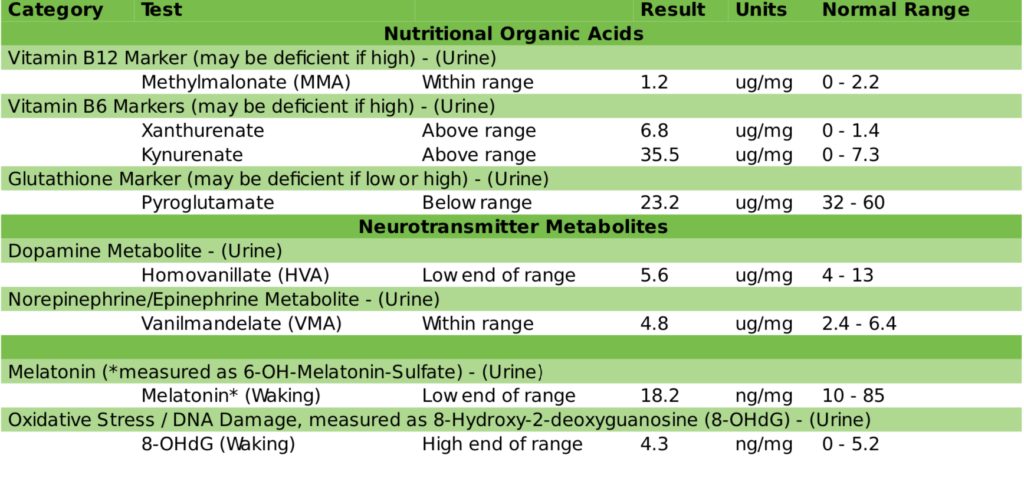
Whoever gets your test for you, it is urine, that’s the way Organic Acids are measured. Here’s what you get in the OATs test, and so much more! I love it and highly recommend it if your issues are long standing. See above. Talk to your physician very openly and allow him/her to experiment with different treatments. Also seek natural options, they work. Here’s an example of the metabolites that are tested in test I just mentioned.

Suzy Cohen, RPh, has been a licensed pharmacist for over 30 years, blending conventional medicine with natural approaches to help people feel better and live healthier. She is the founder of Script Essentials, a supplement company known for targeted, custom-formulated products, some with patented innovations.
With a special focus on thyroid health, functional medicine, and drug-induced nutrient depletion (what she calls “drug muggers”), Suzy is the author of several books including Thyroid Healthy, Drug Muggers, and Diabetes Without Drugs. She also writes a nationally syndicated health column and shares practical, easy-to-understand guidance with readers around the world.
