As a health and wellness blogger with a passion for uncovering lesser-known medical conditions, I recently stumbled upon the intriguing world of misophonia, which literally translates to “hatred of sound.”
It is not an exaggerated sensitivity to noise, nor is it about the volume or frequencies – that would be more along the lines of hyperacusis. A lot of people have sound sensitivity. Also, true misophonia involves more than just irritation from seeing someone eat food and chew with their mouth open – though that is annoying to watch for probably everyone! Importantly, disliking this behavior does not indicate misophonia, again, many people find that disturbing.
It is more complex and it’s a disgust and loathing of certain sounds and the reaction varies from incident to incident, and from person to person. It can cause nervousness, anxiety, sensation of feeling trapped or out of control. It can lead to a physical or verbal outburst, and it can cause estrangements and distance between people, even loved ones. If you scroll down below, I’ve listed a few examples of how this condition gets rooted early on, and how relatives can become triggers.
If I have my facts correct, a trigger warning was issued to ticket holders for a play in London because the actors would be eating oranges on stage. They were concerned they were going to agitate the misophonics in the audience. I’ve never heard of such a warning for a play before, which made me wonder about the severity and prevalence of this condition. Seeing an orange isn’t a trigger, it’s more the sound of slurping, eating and chewing!
For the rest of people who are unaffected (and I am in the unaffected category in case you’re curious), these everyday noises are overlooked. I’m referring to sounds like chewing food, popping or chewing gum, breathing, sniffling, or the sound of a crying baby, also gulping, burping, and possibly opening up the wrappers of snacks. See Table 1 below for a more comprehensive list of sounds that trigger misophonics.
Most of us might hear everyday noises like chewing or tapping and barely register them. Even if they’re not exactly pleasant, they don’t bother us much. For some, people these noises might be mildly annoying but they slip under the radar, forgotten almost as soon as they occur. However, for those with moderate to severe misophonia, these same sounds can be utterly debilitating or provoke intense rage.
Intrigued by the profound impact that everyday sounds can have on us, and how sounds that I don’t even notice trigger severe emotional reactions for others, I felt driven to research, and write this article. I hope it will help you or someone you love learn more and get better. I actually wrote a second article on this condition regarding holistic, natural treatments that work, 9 Herbal and Probiotic Strains that Help Misophonia.
Let’s dive deeper now.
What is Misophonia?
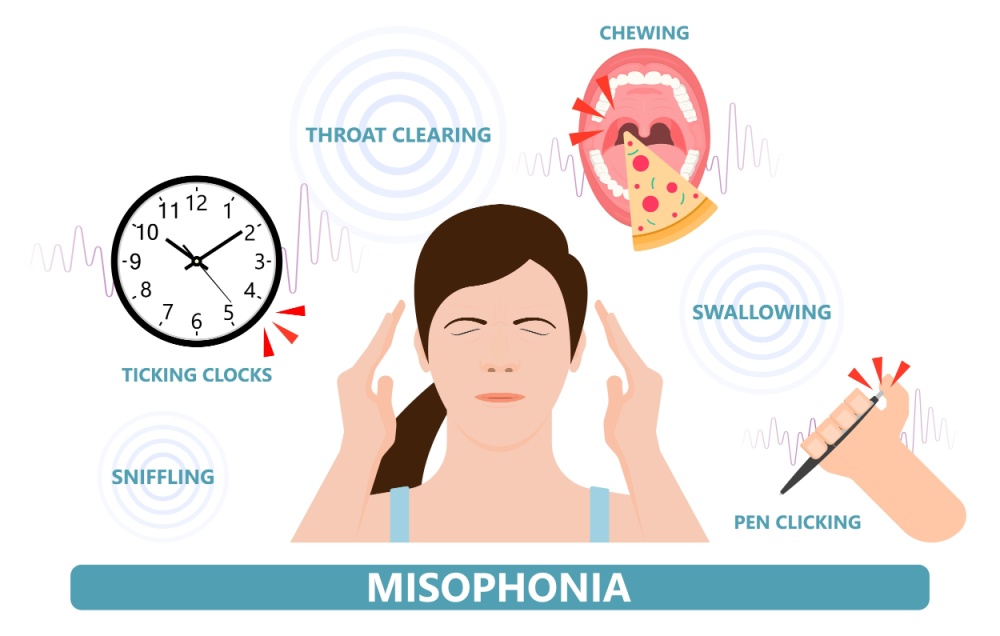
Misophonia, a term that translates to “hatred of sound,” is a condition that triggers intense emotional reactions to ordinary sounds such as coughing, eating, chewing, or breathing. These sounds, seemingly innocuous to most, provoke feelings of either anger, disgust, or anxiety in those affected by misophonia. It’s often misunderstood and under-researched, but it significantly impacts the quality of life for those who suffer in silence.
Misophonia is primarily associated with sounds related to bodily functions – eating, breathing, and chewing are common triggers. However, repetitive sounds like keyboard typing or ticking clocks can also evoke strong reactions.
The response is not just mild annoyance, instead it can be so debilitating that it makes a person want to isolate, affecting social interactions, relationships, and every single daily activity.
Symptoms
Misophonia symptoms can vary widely among individuals but generally include:
- Emotional Reactions: Extreme irritation, anger, panic, or distress upon hearing triggering sounds such as chewing, breathing, or repetitive tapping. It can be the sound of their own chewing, not just others.
- Physical Reactions: Sweating, muscle tension, or even becoming physically aggressive or needing to get away from the sound. Leaving the room is common. Not participating when expected to is also common.
- Anticipation and Avoidance: Increased sensitivity and anticipatory anxiety about situations where triggering sounds may occur, leading to social withdrawal or avoidance behaviors.
Here are 5 different examples of how this condition manifests:
“You know, it’s the strangest thing. I hate the sound of chewing. Even someone munching on chips or slurping soup can drive me up the wall. It’s not just annoying—it feels like I’m being poked repeatedly. Makes me want to end the relationship!”
“I might seem a bit odd when I wear headphones during lunch in the office. It’s because the sound of chewing really gets to me. It’s more than a little irritating it actually makes me super anxious.”
Opening Up in a Support Group:“Hi everyone, I’m really glad to be here. Dealing with misophonia can be so isolating. The sound of a clock ticking or someone breathing heavily can ruin my entire day. It’s like a switch flips in my head and I can’t focus on anything else.”
Discussing with a Family Member: “Mom, I really need you to understand why I always eat alone. It’s not that I don’t enjoy family time, but the sound of everyone eating, the clinking of forks and knives, it overwhelms me and I find it unbearable.”
“I love going out, but the sound of people chewing or background music played through bad speakers can send my stress levels through the roof. I hate that it controls so much of my social life.”
Trigger Sounds
People with moderate to severe cases of misophonia experience severe emotional reactions to certain everyday sounds, which can vary widely among individuals. The most commonly reported annoying sounds for those with misophonia include:
- Eating Sounds: Chewing, crunching, slurping, burping, or utensils hitting or scraping against plates.
- Breathing and Nasal Noises: Sniffling, breathing heavily, or nose whistling.
Nose-blowing would fall into this category too. Speaking of, you might want to take a few minutes to read my other article on this topic, Allergies and your Genes. - Vocal Sounds: Lip-smacking, throat clearing, or the sound of certain consonants like “s” or “p.”
- Repetitive Tapping: Fingers tapping on a surface, keyboard typing, or tapping feet.
- Other Mundane Sounds: The ticking of a clock, the clicking of a pen, or the rustling of papers.
Table 1: Trigger Sounds (Journal of Neuroscience)
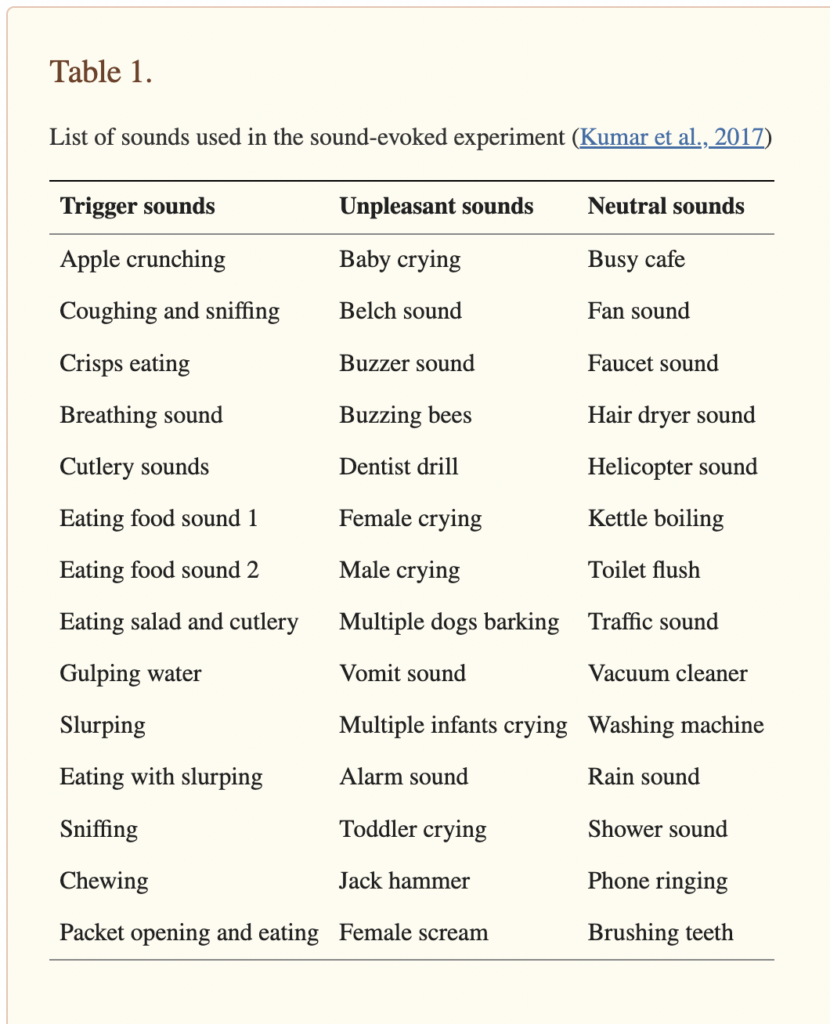
Table 1 from “The Motor Basis for Misophonia”
Risk Factors
While the exact risk factors for misophonia are not fully understood, several elements may increase the likelihood of experiencing this condition. There could be a family history, it could be a co-morbid condition occurring with anxiety, OCD, Tourette, BIPOLAR DISORDER, autism, and others. Hormones that change in late childhood or the early teen years also appear to influence onset. It seems that women are slightly more affected than men, but it’s not a landslide.
Some theories suggest that misophonia could be triggered by an initial emotional trauma that was associated with a specific sound that then carries on through life. The idea that misophonia might be triggered by certain events is intriguing. Here are 5 examples:
- Childhood Experience: Imagine a child who experiences their parents fighting or arguing during dinner and it’s accompanied by the clinking or breaking of dishes. Later in life, the sound of dishes clinking or utensils on the dishes might trigger anxiety even if all is well in their current reality.
- School Incident: A student might develop misophonia after being called out or embarrassed or humiliated in a classroom and as an example, or maybe they got called to the principal’s office. Anyway, the clock is loudly ticking during this and now that sound becomes a trigger. See the pattern. Let me think of a few more.
- Medical Procedures: You might have had a painful injection or exam, or maybe had a frightening medical procedure or wheeled into the surgery center (there are so many), but anyway, hearing the beeping of machines or clicking of a dental drill then becomes a lifelong trigger. This is extremely common, and while it’s not misophonia it is a relatable sound-induced form of anxiety that all of us probably recognize and deal with.
- Accident Scenes: If an individual was involved in or witnessed a traumatic accident where a specific noise was prominent, like tires screeching or shattered glass, these sounds could later become triggers. Again, not related to misophonia (which usually has more to do with bodily functions), but still relatable.
If you are interested in another article I wrote about this, check out, 9 Herbal and Probiotic Strains that Help Misophonia.
If you are interested in an article I wrote regarding PTSD (Post-Traumatic Stress Disorder), CLICK HERE.

Neurological Underpinnings and Mental Health Correlations
Research into misophonia is still in its early stages, but several studies have begun to shed light on its neurological basis. One key study suggests that it involves abnormal connectivity in the brain’s auditory cortex and limbic system, areas responsible for processing sound and emotion, respectively. Other experts believe it is low serotonin (or serotonin resistance) which I do agree with. We already suspect from numerous studies that serotonin deficiency can make some people more impulsive, possibly violent and AGGRESSIVE. Furthermore, different research into serotonin deficiency plots a possible link to another condition, Tourette’s syndrome. Learn more about that here: tourette.org.
And finally, another significant aspect of misophonia is it often occurs with OCD. Learn more about OCD HERE.
 In 2018, there was an analysis, and the research was published in the Journal of Obsessive-Compulsive and Related Disorders (JOCRD) which explored this. It involved over 800 participants who took online surveys about sound sensitivities and related psychological factors.
In 2018, there was an analysis, and the research was published in the Journal of Obsessive-Compulsive and Related Disorders (JOCRD) which explored this. It involved over 800 participants who took online surveys about sound sensitivities and related psychological factors.
The findings indicated a close connection between misophonia and OCD (which involves persistent, unwanted and usually distressing thoughts). The study also showed that OCD symptoms help explain how anxiety sensitivity relates to misophonia severity.
Sussex Misophonia Scale
In a newer 2022 paper from Frontiers in Psychology, the same correlation was found after assessing 142 children (between the ages 10 to 14). They used a newly developed “Sussex Misophonia Scale” for adolescents to identify kids who were already experiencing symptoms of misophonia. It was a questionnaire, no blood was taken, or labs drawn.
Anyway, the results were telling and concur with the 2018 study: Kids with misophonia showed much higher levels of anxiety and OCD traits. They also reported poor satisfaction with life and worse health-related quality of life. Interestingly, creativity was not impacted.
In 2023, researchers in India studied prevalence, they wanted to know exactly how common this is in high school students. There was an intriguing PAPER published in Indian Journal of Otolaryngology and Head & Neck Surgery. The research involved 597 students, aged 14 to 16, who completed the Misophonia Assessment Questionnaire to assess their reactions to specific sounds. Results showed that 34.67% of these students experienced misophonia, with classifications ranging from Mild to Severe.
The findings reveal that misophonia is more prevalent among high school students compared to college students in India, possibly due to the emotional and developmental changes typical during adolescence. This study underscores the need to address misophonia during these formative years to support adolescent well-being.
Neurotransmitters and Myelin
Many people have heard of myelin (the protective sheath around nerve fibers) as it pertains to Multiple Sclerosis (MS) and a loss of myelin progressively occurs. People take B12 shots sometimes to improve myelin synthesis.
In the case of misophonia, it appears to be opposite of what occurs with MS. It may be excessive myelin formation that is in the auditory pathways, not the destruction of it.
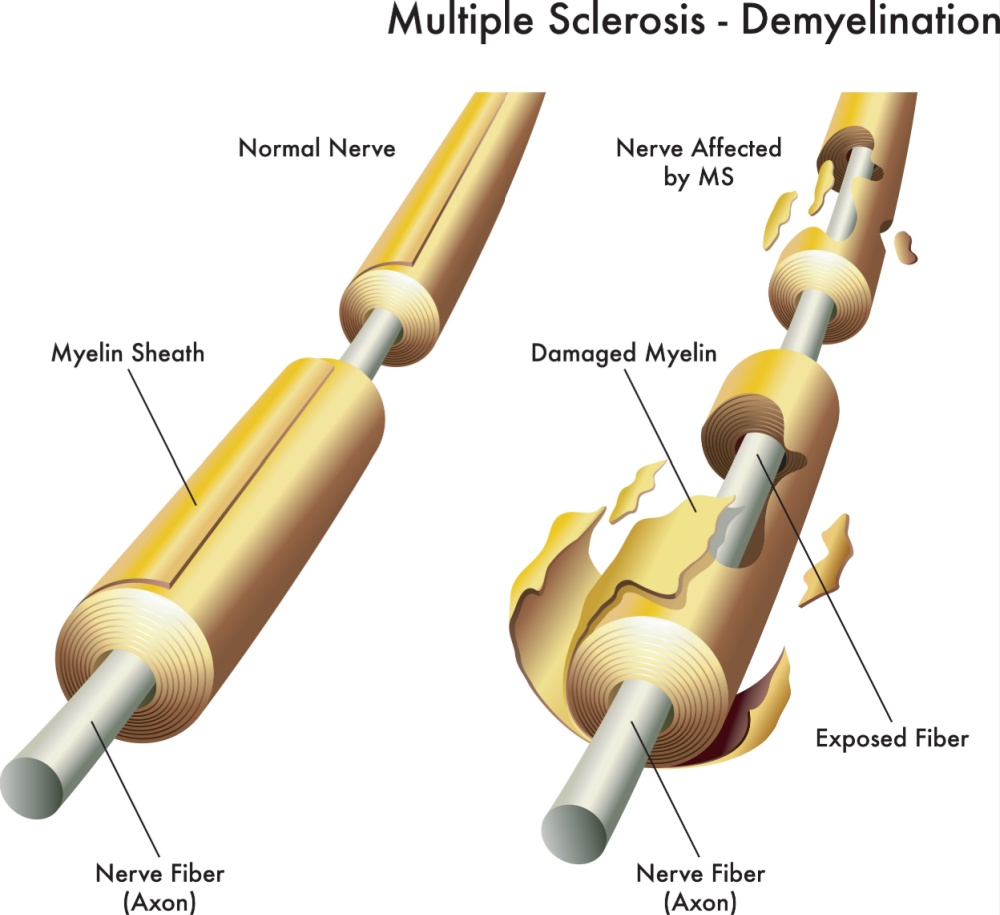
The theory is that overproduction of myelin enhances the speed and sensitivity of sound signal transmission. It’s like too much myelin sets the stage for ‘super hearing’ in people with this condition.
But myelin doesn’t explain the mental health aspect of it, just how the sound might be taking the forefront of their life versus it being background noise like it is for most people.
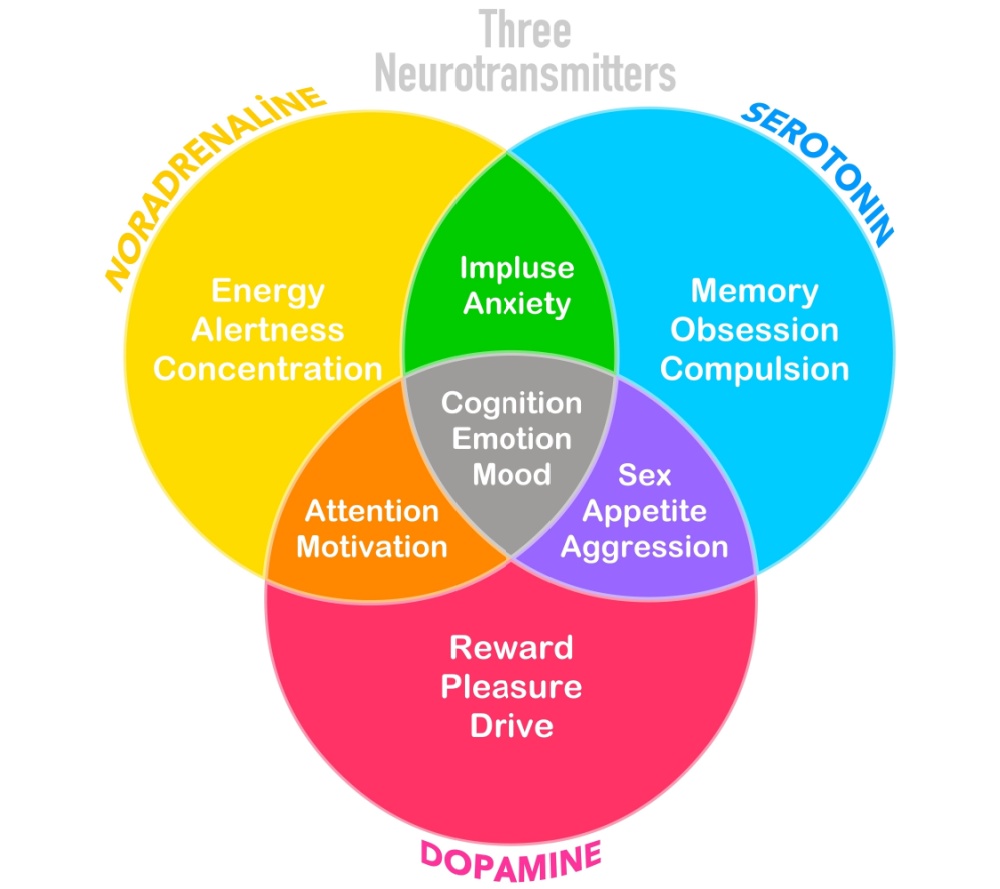
Misophonia is linked to imbalances in neurotransmitters, either an excess or deficiency of serotonin and/or dopamine. It would be so much easier to treat if we could say too much of this, or too little of that causes it. But neurotransmitters don’t work that way.
They are in constant flux being synthesized in one place, released over there, traveling over here and then degraded in other parts of the body. It’s way more than a see-saw with neurotransmitters. But the point is, they could play a role in the heightened sensitivity to sound and the over-reaction of it. The levels of these hormones have a U-shaped relationship with how your brain processes and responds emotionally to sounds. This means that too much or too little can throw off the way sounds are perceived and emotionally handled. It’s all about keeping these hormone levels in balance for optimal brain function.
Autoimmune Disorders and Hyperthyroidism
Recent research is beginning to explore the potential links between misophonia and autoimmune disorders, including hyperthyroidism (Graves’ disease or Hashimoto’s thyroiditis), Lyme disease, lupus, and others.
People being treated for high levels of thyroid hormone sometimes report misophonia and other symptoms of heightened sensory sensitivity. They can experience mild hyperacusis or misophonia. Read my article, 10 Key Symptoms Of Hyperthyroidism: Understanding The Overactive Thyroid.
Why Do These Sounds Bug You So Much?
Scientists have found that misophonia isn’t just about your ears being sensitive. It actually has a lot to do with the brain, especially the parts that control movement. In 2021, there was a STUDY conducted that showcased the fact that it’s not just your ears that notice someone chewing, your brain mirrors the activity and it’s like your brain acts like it’s chewing too!
This doesn’t happen when you actually chew, but the brain of patients with misophonia acts as if it is copying those chewing motions that it sees. That’s why the sound can provoke such intense reactions – it’s like their brain is overreacting to what it hears and sees due to mirroring.
In the study, researchers found that the brain areas that handle hearing sounds are super connected to the areas of the brain that control movement which go into overdrive once they hear the offending sound. And most importantly, at least in terms of trying to treat the condition, it’s the part of our brain that responds with movement that might be causing these strong reactions.
Understanding this could change how we help people with misophonia. Instead of just trying to block out the sounds or avoid them, treatments should focus on controlling the overreaction. Things that help the brain to chill out a bit when it hears trigger sounds would be the focus. To that end, the basal ganglia and CSTC are both involved in movement – and both of those sections are involved in Tourette syndrome. Let’s dive a bit deeper because these two conditions overlap occasionally.
Neurological Overlap with Tourette Syndrome
Tourette Syndrome is a neurological disorder characterized by involuntary, repetitive movements and vocalizations known as tics. These tics are sudden, brief, and can vary widely in type and severity, often worsening with stress and improving with concentration or focus.
Both misophonia and Tourette syndrome involve dysregulated neural circuits, particularly in areas of the brain that are responsible for sensory processing, emotional regulation, and motor control:
- Basal Ganglia: This critical cluster of brain cells is key to how we control our movements and regulate our emotions. In conditions like Tourette syndrome, the basal ganglia are often at the heart of the involuntary tics—those sudden, repetitive movements or sounds that characterize the disorder. Interestingly, this same area may also play a significant role in misophonia, where it’s thought to amplify the way we process sounds and our emotional reactions to them. This similarity suggests there could be a deeper connection in how these conditions affect sensory and emotional processing in the brain.
- Cortico-Striatal-Thalamo-Cortical (CSTC) Circuits: These neural loops are all about filtering the information our senses pick up and how we respond to it physically. In Tourette syndrome, when these circuits don’t work as they should, it can lead to those hard-to-control tics. For those with misophonia, a similar disruption might make it tough to tune out or process certain sounds normally, triggering intense emotional and physical reactions that can be overwhelming.

- Limbic System: Nestled deep within the brain, this system, which includes areas like the amygdala, is essentially our emotional command center. Both misophonia and Tourette may involve unusual activity in this part of the brain, which could explain the strong emotional responses triggered in both conditions. Whether it’s a sound that suddenly feels unbearable in misophonia, or the emotional challenges in Tourette syndrome, it’s clear that the limbic system plays an important role.
Both misophonia and Tourette syndrome involve involuntary reactions to stimuli. People with misophonia may feel an urgent need to escape from sounds that trigger intense emotional responses, while those with Tourette Syndrome experience compelling urges to perform tics, often in response to specific sensory inputs. These behaviors highlight the brain’s complex response to discomfort.
Medications That Might Worsen Misophonia Symptoms
What if something you already take is making you suffer worse? The following information is hard to find, but I’ve created a list in case you want to see if you take anything here. Of course, do not suddenly stop a medication (some have to be tapered or you can get a seizure!), so just work with your doctor if you want to switch, stop or pause it. Here are the most common offenders in terms of worsening misophonia:
- Stimulants: Medications such as those used to treat ADHD (ie amphetamines) can increase alertness and sensitivity, potentially heightening awareness of and reactions to triggering sounds.
- Anxiolytics and Sedatives: This one is wild because these drugs are also used to treat misophonia! But some people have the opposite reaction due to their individual chemistry. So while these are often prescribed to reduce anxiety, their effects on the nervous system might paradoxically heighten sensitivity to sounds!
- Antidepressants: Another paradox! Some people may experience changes in emotional regulation or sound processing when they start these drugs, or change dosages. SSRIs (selective serotonin reuptake inhibitors), like citalopram, paroxetine, sertraline and others influence serotonin levels in the brain, and dopamine balance which could then modify the way sounds are processed and perceived (possibly making misophonia worse over time). Also, these drugs do not increase serotonin production, they essentially make it last longer. This means that the condition could worsen with time because the drugs don’t work as well after being on them for awhile.
Non Pharmacologic Treatments (as of May 2024)
If you have this condition, see a qualified doctor because the below suggestions are just that – ideas to help educate you and point you in the right direction. Also, there is no one-size-fits-all treatment for misophonia, but several strategies can help manage symptoms:
- Sound Therapy: Using background noise or white noise to mask triggering sounds. There are phone apps available now, and devices galore that work like this.
- Cognitive Behavioral Therapy (CBT): Helps patients reframe their thoughts about triggering sounds and develop coping strategies.
- Tinnitus Retraining Therapy (TRT): Although traditionally used for tinnitus, TRT combines sound masking and therapy to reduce the patient’s reactions to specific sounds. According to this PAPER, misophonia “does have shared genetic etiology with tinnitus.”
- Psychoeducation: Educating patients and families about misophonia can help them understand the condition and reduce stress related to symptoms.
- Neurofeedback: I was actually trained and certified to be a neurofeedback therapist in the late 90s but I don’t practice. I’m listing this because a therapist in your area may be able to provide help for this misophonia, if only to reduce feelings of anxiety, which then reduce cortisol and blood pressure.
Therapeutic Medications to Consider
Medications should be considered to address underlying issues such as anxiety or depression in serious cases. These conditions can exacerbate misophonia symptoms.
There is nothing specifically FDA-approved for the treatment of misophonia, however, medications that treat other mental health disorders may work. For example, drugs used to treat OCD, Tourette syndrome, schizophrenia, anxiety and/or depression will target the proper neurotransmitters.
Each medication works differently, so it becomes a bit of trial and error for a patient to work out with the doctor. If you tweak it just right, over time, you should be able to reduce underlying issues that contribute to the condition. Specifically, drugs that either increase GABA activity or serotonin could work.
- Antidepressants (ie SSRIs like fluoxetine, sertraline): These manage anxiety and depressive symptoms, potentially reducing the intensity of misophonia reactions. But it could also go the other way, and make it worse!
- Benzodiazepines (ie diazepam or clonazepam): Used sparingly, these can provide relief from acute anxiety and agitation triggered by specific sounds, although they carry a risk of dependence and tolerance.
- Beta-Blockers (ie propranolol): These are sometimes used off-label for performance anxiety and may help reduce the physical symptoms of anxiety related to misophonia.
- Anticonvulsants (ie gabapentin or pregabalin): While typically used to treat epilepsy, these have also been used to manage sensory disorders and might reduce the intensity of auditory triggers by enhancing GABA (gamma -aminobutyric acid). They work by reducing neuronal excitability.
- Atypical Antipsychotics (ie risperidone): In cases where other treatments have failed, these may be considered to help regulate mood and reduce irritability.
Endocannabinoids and Cannabis: Does Pot Work?
Everyone has a ‘pot’ center in the brain, it’s an important metabolic pathway in the body called the endocannabinoid system. This is different than your CNS (Central Nervous System).
The endocannabinoid system regulates mood, stress, pain and other important neurological pathways that control seizure threshold. This system includes naturally occurring compounds called “endocannibinoids” in your body that bind to cannabinoid receptors (primarily CB1 and CB2 receptors) and perform similar functions as compounds found in cannabis (marijuana).
Specific research on this herb for the treatment of misophonia is sparse and only anecdotal. However, there could be potential benefits worth exploring under the guidance of an expert, keeping in mind the strain, the balance of sativa to indica, the time of administration, dose, etc. I simply don’t know enough about it to offer guidance, so work with a practitioner who is familiar with all of these factors.
I wrote another article on this topic, The Crazy History of Medical Cannabis and 5 Potential Uses.
Summary
Misophonia is a condition where everyday noises like chewing, coughing, or breathing can provoke intense emotional reactions. Unlike the mild annoyance these sounds might cause in most people, those with misophonia find them overwhelmingly irritating and distressing. Although the exact causes are not fully understood, it involves atypical connections in the brain’s auditory cortex and limbic system. This affects how sounds are processed and emotionally perceived. There’s also speculation that imbalances in neurotransmitters such as serotonin and dopamine might play a role.
Interestingly, misophonia shares neurological characteristics with Tourette syndrome, especially in the involvement of the basal ganglia and cortico-striatal-thalamo-cortical circuitry. These areas are essential for processing sensory things like sight, hearing, touch, taste, and smell. Also involved is our ability to plan, initiate movement and walk.
It all suggests that treatments for Tourette syndrome may help misophonia too. Understanding the links between misophonia and other neurological and psychological conditions including anxiety, OCD and Tourette syndrome can improve our treatment approaches.

Suzy Cohen, RPh, has been a licensed pharmacist for over 30 years, blending conventional medicine with natural approaches to help people feel better and live healthier. She is the founder of Script Essentials, a supplement company known for targeted, custom-formulated products, some with patented innovations.
With a special focus on thyroid health, functional medicine, and drug-induced nutrient depletion (what she calls “drug muggers”), Suzy is the author of several books including Thyroid Healthy, Drug Muggers, and Diabetes Without Drugs. She also writes a nationally syndicated health column and shares practical, easy-to-understand guidance with readers around the world.
