For years we have heard that statins are the gold standard pharmacological treatment for high cholesterol. But there’s more to the story because those drugs, introduced in the 1980’s when I was a young pharmacist, do not vacuum the cholesterol in your blood vessels. They only block endogenous production by your body, and in doing so, they can lead to uncomfortable side effects due to the drug mugging effect of ubiquinol. Ubiquinol is an antioxidant you make in your body, and it’s also one you can buy as a dietary supplement. Ubiquinol is the activated form of CoQ10.

Here’s my stance on the subject of “cholesterol.” This is an all-encompassing umbrella term that refers to many different ‘pieces and parts.’
I do not think cholesterol is bad, on the contrary. However, the ratios of the pieces and parts (all the different particles) should remain in a healthy balance. It is not cholesterol itself that leads to heart attacks… it couldn’t possibly be or we’d all be dead by virtue of the fact that we all have cholesterol in our body! It is every present every second of the day, and required for survival. Your liver makes 3/4 of your total cholesterol.
So then what is it?
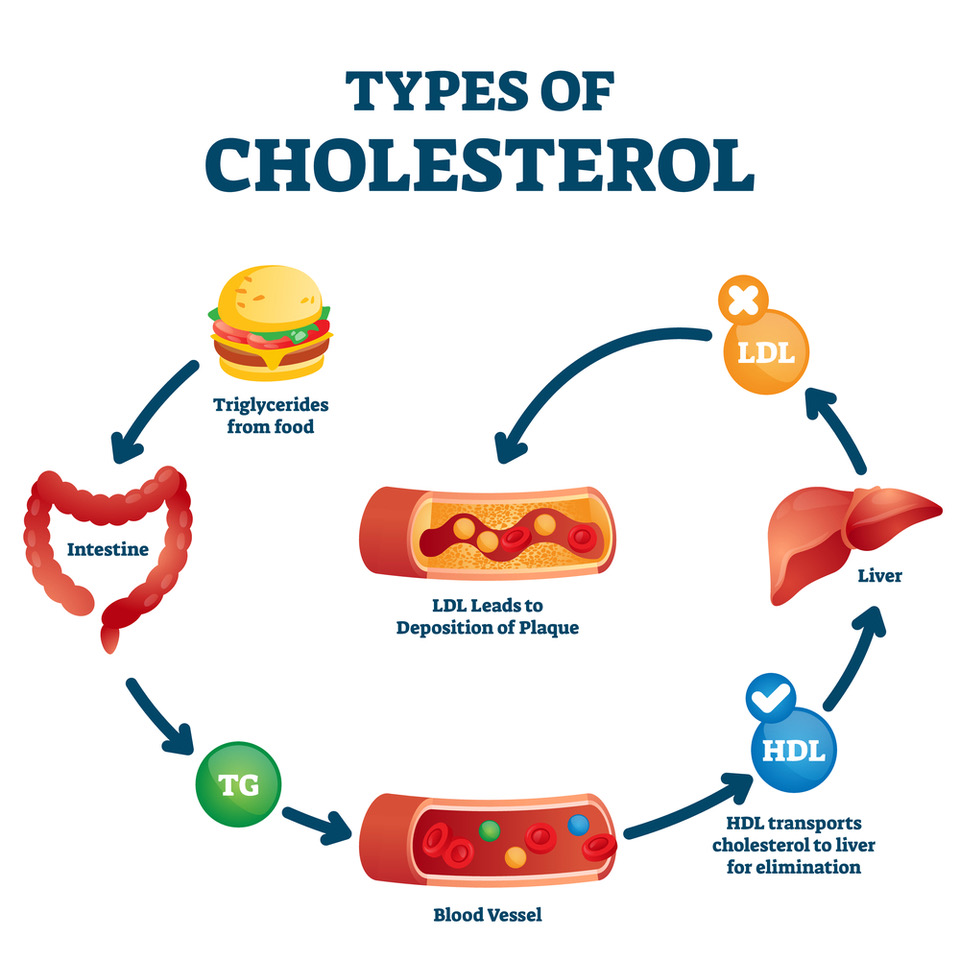
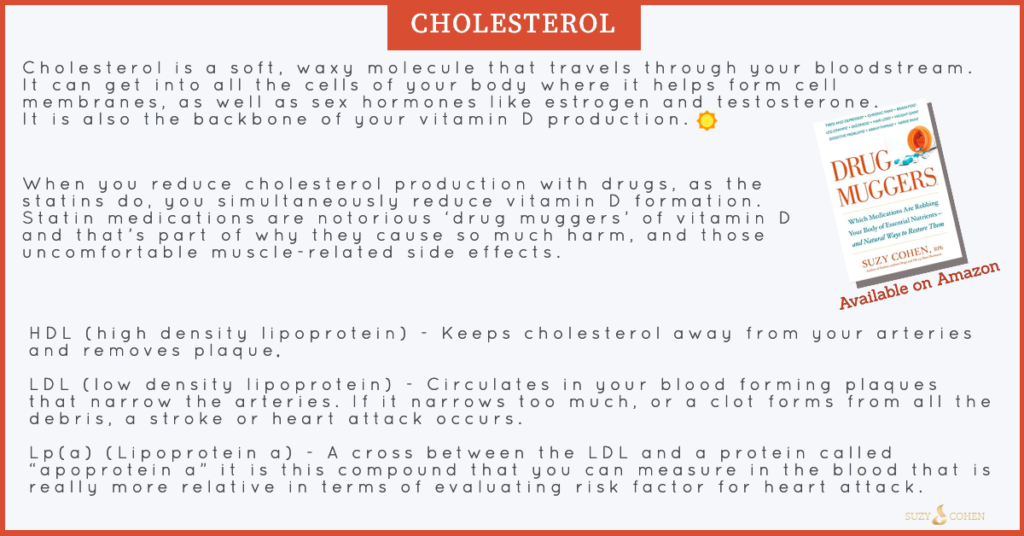
Total cholesterol is not the problem, it’s more the imbalanced ratio of certain particles. There are many particles of cholesterol, but the two most famous ones are LDL and HDL. The LDL particles are the dense “bad” ones and the HDL are the good ones. Keeping this superbly simple, you want to keep the HDL level high, and reduce the amount of LDL to have the best health outcomes.
Over the years, the medical system have lowered the target reference ranges for cholesterol, while raising the HDL ranges… so much so, that according to those desirable numbers, practically all Americans above age 3 now needs a statin! 😜 This is a bit ridiculous, and very uncomfortable to reduce cholesterol production so greatly! You need cholesterol and I’ll tell you why right now.
Here’s a link to my Drug Muggers book if you’re interested in drug nutrient depletions for any medication you take. You can also read an article I wrote on this subject called “Shocking Cholesterol News.“
Meet the PCSK9 Inhibitors a.k.a. Cumab Drugs
Even though I prefer natural approaches to medical situations, as a pharmacist I can at least offer you my perspective on the newest therapeutic tool for high cholesterol, specifically LDLs (which you want to reduce). This new category of meds are referred to as the PCSK9 inhibitors. Let’s talk about those more in depth, but first let me assure you those drugs do not deplete CoQ10 like the statins, so their side effects are different.
The PCSK9 Inhibitors are a new category of drugs that are going head-to-head with blockbuster statins! The specifically reduce LDLs and they are given by self-injection, they are not pills that you easily swallow. The injection comes from the pharmacy as a pre-filled pen and you inject it SQ (subcutaneously) every 2 weeks, akin to the way some diabetics inject insulin.
You as a human being carry a gene called “PCSK9” which stands for “proprotein convertase subtilisin kexin type 9” and it is found on chromosome 1.
This is a gene that provides the blueprint to build a protein in your body (by the same complex name above), which controls the amount of cholesterol that goes into your bloodstream. This PCSK9 protein controls the quantity of LDL receptors on the outside surface of every cell. These receptors are doorways, and they hug in (bind) LDL particles which are the primary taxi cabs and carriers of cholesterol in your blood. These receptors are very important, and they play a critical role in regulating blood levels of cholesterol.
LDL receptors are particularly abundant in your liver cells, because it is this specific organ that is responsible for removing all the extra cholesterol in your body that you don’t need. For that matter, the number of LDL receptors on the liver cells is precisely what determines how fast you get the cholesterol out of your bloodstream! The more LDL receptors you have, the better.
The PCSK9 protein in your body is what destroys those LDL receptors before they reach the surface of your cells, and this means more cholesterol stays in the bloodstream.
If you had more LDL receptors on the surface of your cells, then the LDL would hug them (bind to them) and get the heck out of your bloodstream. (Excellent, that’s what you want). And this is in fact what the PCSK9 inhibitors do —> they prevent the destruction of LDL receptors and in doing so, more remain on the cell surface, therefore the LDL can bind to it, thus leaving your bloodstream. Using the famous ‘key in lock’ analogy, the LDL is the key and can put itself into more locks (receptors) and get out of the blood where they clog the arteries and serve as a bottleneck in the blood vessel. Then, ultimately, your LDL blood levels go down, which is the goal for many cardiologists trying to lower your cholesterol. They want that LDL to go down!
If your liver is damaged from alcohol consumption, or from insufficient liver enzymes and antioxidants, you compromise processing and detoxification of cholesterol.
So the PCSK9 inhibiting drugs prevent your liver’s LDL receptors from breaking down. Like statins, they increase availability of LDL receptors to lower the LDL particles. But in the clinical trials published (and there may be others that remain unpublished for now), the new category of PCSK9 inhibitors appear to conduct this task better.”
There are two new medications in this category:
Praluent® (chemical name: Alirocumab)
Repatha® (chemical name: Evolocumab)
[See the names here, they both end in “cumab” so since it’s easier for the sake of reading my article, I will refer to this category of drugs as cumab drugs, or the cumabs. That’s not an official nickname, it’s just for reading ease and I’ve made it up!]
According to clinical trials, the PCSK9 inhibitors (I mean the cumab drugs!) reduce LDL cholesterol by about 60% which in turn could reduce cardiovascular risk (ie heart attack, chest pain, unstable angina, and stroke) by upwards of 15%.
Who might this work for?
1. Anyone who has elevated LDLs that are resistant to other methods of treatment.
2. Those who don’t mind self-injection.
3. People with Familial Hypercholesterolemia (FH), this is a genetic condition that could occur due to a SNP (polymorphism) in the PCSK9, which again encodes the blueprint to make the protein by the same name, which has to do with your LDL receptor sites. That said, Familial Hypercholesterolemia does not always occur due to PCSK9 SNPS, it may also be due to mutations in the APOB, LDLR or LDLRAP1 genes. I so love to talk about genes, and study them constantly, but this article isn’t the right time or place to delve too deeply in these. I will again some other day. By the way, statins do not work well in cases of this condition.
4. People with a history of major cardiovascular insult, such as an MI (heart attack) or stroke, or even a small aneurysms. There is a highly significant association between levels of LDL cholesterol particles and aneurysms. The idea is that the LDL is acting badly, and increasing levels of a pro-inflammatory cytokine called MMP-9 and this is one initiating factor behind aneurysms.
I only mention this because the current presidential candidate, Joe Biden suffered from two aneurysms back in 1988, and the “cumab category of drugs” (PCSK9 inhibitors) may be of use since they down-regulate LDL levels which crank up MMP-9.
So if I was consulting for our 2 candidates, I would suggest this:
President Donald J. Trump – Take the statin along with CoQ10 and Vitamin D because he has high cholesterol.
Former Vice President Joe Biden – Take the Cumab drug because it specifically targets the LDL receptors, along with niacin because of his past medical history.
Maybe someone on their team will see this and get a message to each of them.
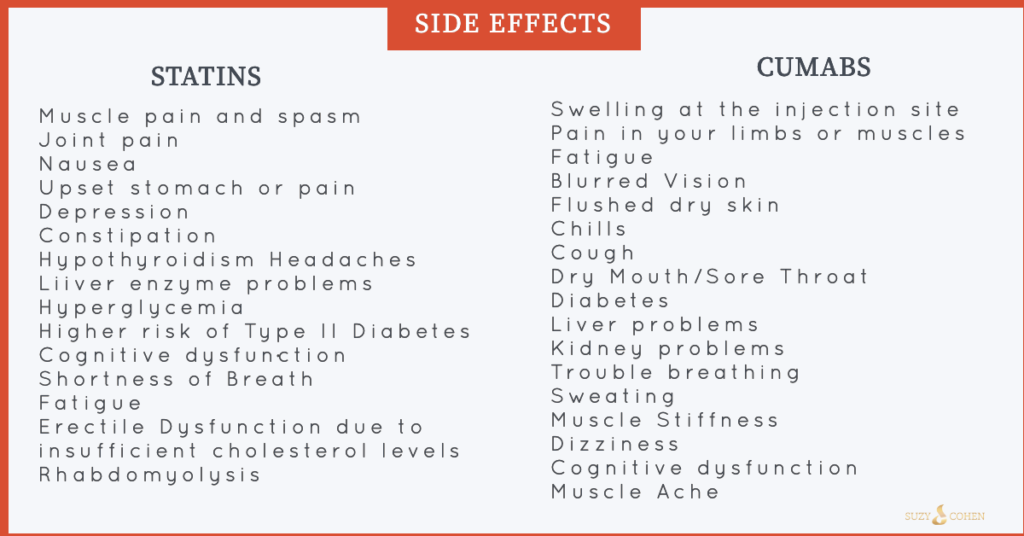
5. People who cannot tolerate statins due to the side effects. The muscle pain, CoQ10 depletion, mood destabilizing effects and impact on memory are sometimes just too much to handle. Restoration of depleted ubiquinol (the activated form of CoQ10) is useful and helpful, as well as a new category of medications such as the cumabs.
6. A person who is at high or imminent risk for a stroke or heart attack, who remains uncontrolled with statins, exercise and diet.

Perhaps you are wondering.
Are the cumabs better than the statins?
We can’t say for sure, no one knows because they’re brand new drugs. The trials took about 2 or 3 years, and then the rest of the studies happen on the population. So we’ll know more in a few more years.
Is taking a cumab preferred to losing weight and eating a clean, mainly green diet?
Remember, diet is the #1 way to control cholesterol ratios and it works! Exercise matters greatly and so does protecting your liver as well. In my opinion, no drug is better than you doing the work yourself and getting your own body to produce perfect cholesterol ratios. It’s always better to have a good BMI, and eat a clean diet, and the reason is because your only side effect from that, is better health!
Do the PCSK9 inhibitors (the cumabs) actually reduce the risk of death?
Yes, they do have that ability. They not only improve mortality, but can reduce morbidity through reduction of MMP-9 and other pro-inflammatory cytokines. You have to determine the risk to benefit ratio, and make an informed decision for yourself. Have a conversation with your cardiologist, see holistic practitioners, commit to some lifestyle changes and of course, take care of your “filter organ” as in your liver. If you can’t filter out toxins, they build up in your body, and in your bloodstream and cause disease.
Differences: PCSK9 inhibitors vs. Statins
PCSK9 inhibitors (the “cumabs”) as well as statins reduce LDLs, but the cumabs are better at it!
They do not suppress CoQ10 (or Ubiquinol) because they do not block the enzyme called HMG-CoA reductase like the statin do. When you block that enzyme, you reduce total cholesterol production. Statins also work by helping your body to reabsorb any left over cholesterol that has gathered on the inside walls of your blood vessels, PCSK9 does not do this.
Statin side effect profile is different than with PCSK9 inhibitors.
The PCSK9 drugs have no long-term safety data.
Statins are far less expensive than cumabs, but insurance should cover if you have the diagnosis of FH. As for prices… the average annual price right now is $14,000 per year for cumab therapy. Statins vary, but are in the ballpark of $800 – $2000 depending on which drug, and the dosage.
Statins are oral drugs whereas cumabs are injection.
Statins reduce cholesterol by reducing production of it in the liver cells. Cumabs reduce cholesterol by making your liver get rid of it more efficiently.
Other Methods of Reducing Cholesterol
I did not mention Zetia® (ezetimibe) or binders such as cholestyramine (Questran® or Locholest®) or colesevelam (Welchol®) or others. Since those are working through the intestinal tract, they are not at all helpful with LDL receptors in your liver tissue. Because they have a different pharmacological mechanism of action, they could be used in conjunction with either a statin or cumab. Other adjunctive therapies for your consideration include red yeast rice, hawthorn, beta glucan, glucomannan and fish oil. Talk to your doctor about what’s right for you. Keep in mind that she/he will not know what a “cumab” is, that’s my nickname for this category of FDA-approved medications. You’ll need to refer to them as PCSK9 inhibitors. Don’t ask for them if you are needle shy, remember they require injection.
Finally, cholesterol ratios are not the best way to assess heart attack risk in my opinion. Cholesterol levels are sometimes irrelevant meaning people with perfect numbers still suffer a heart attack or stroke. So again, the numbers aren’t the best way to assess your heart attack risk. They should be assessed as part of a bigger work up, with LDL and HDL ratios, and the particle size and numbers/ratios… those absolutely do matter, but total cholesterol values do not matter that much because you do not know the particle sizes.

For example, the amount of HDL to total cholesterol matters. So the ratio HDL/cholesterol is a number you can determine. It should be above 25% ideally. Grab your lab work and a calculator and divide the HDL by the cholesterol and see what your value is. If it’s lower than 25% you want to take supplements to raise your HDL, or alternatively lower your total cholesterol number.
You can and should look at other inflammatory markers in the body such as homocysteine, CRP, Lp(a) which is a biggie. I first wrote about Lp(a) in 2007 in my book, The 24-Hour Pharmacist and some of my articles over the years, yet even today, very few doctors order this test because they are so obsessed cholesterol! Blood pressure matters, as does hormone status. Insufficient levels of DHEA, estrogen and testosterone can all impact your cardiovascular system. These are easily evaluated via blood tests and/or by looking at urine metabolites. In a future article, I will cover natural approaches to reduce your cholesterol. Of course, a healthy diet, exercise and reduction of sugary foods, and smoking will all help.

Suzy Cohen, RPh, has been a licensed pharmacist for over 30 years, blending conventional medicine with natural approaches to help people feel better and live healthier. She is the founder of Script Essentials, a supplement company known for targeted, custom-formulated products, some with patented innovations.
With a special focus on thyroid health, functional medicine, and drug-induced nutrient depletion (what she calls “drug muggers”), Suzy is the author of several books including Thyroid Healthy, Drug Muggers, and Diabetes Without Drugs. She also writes a nationally syndicated health column and shares practical, easy-to-understand guidance with readers around the world.
